CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 5, June 2012
AFRICA
e1
Case Report
Severe haemoptysis due to subclavian arteritis
A LIOULIAS, P MISTHOS, J KOKOTSAKIS, P DROSOS, N KARAGIANNIDIS, D PAVLOPOULOS, M MITSELOU
Abstract
Severe haemoptysis due to infective subclavian arteritis has,
to our knowledge, never been documented. We report a case
of subclavian arterial vasculitis that eroded into the left lung
apex, causing a large intraparenchymal mycotic pseudo-
aneurysm. The patient presented with high fever and blood
expectoration. An emergent left lateral thoracotomy was
performed. The inflamed segment of the subclavian artery
was resected and continuity was restored with a reversed
saphenous vein graft. The postoperative course was unevent-
ful and the patient was discharged on the 10th postoperative
day.
Keywords:
haemoptysis, subclavian artery, arteritis, lung
Submitted 8/6/10, accepted 26/11/10
Cardiovasc J Afr
2012;
23
: e1–e2
DOI: 10.5830/CVJA-2010-096
Seven cases of haemoptysis as the presenting symptom of a
subclavian aneurysm have been published.
1-7
However, severe
haemoptysis due to infective subclavian arteritis has, to our
knowledge, never been documented. We report a case of
subclavian arterial vasculitis that eroded into the left lung apex,
causing a large intraparenchymal mycotic pseudo-aneurysm.
The patient presented with high fever and blood expectoration.
Case report
A 17-year-old male presented with high-grade fever, which
he had had for the previous three weeks, retrosternal pain, and
multiple episodes of severe haemoptysis during the preceding
two days. He was a heroin addict and used the subclavian vessels
as vascular access. He reported that one month previously,
injection at that location was accompanied by severe pain at the
area of the thoracic outlet.
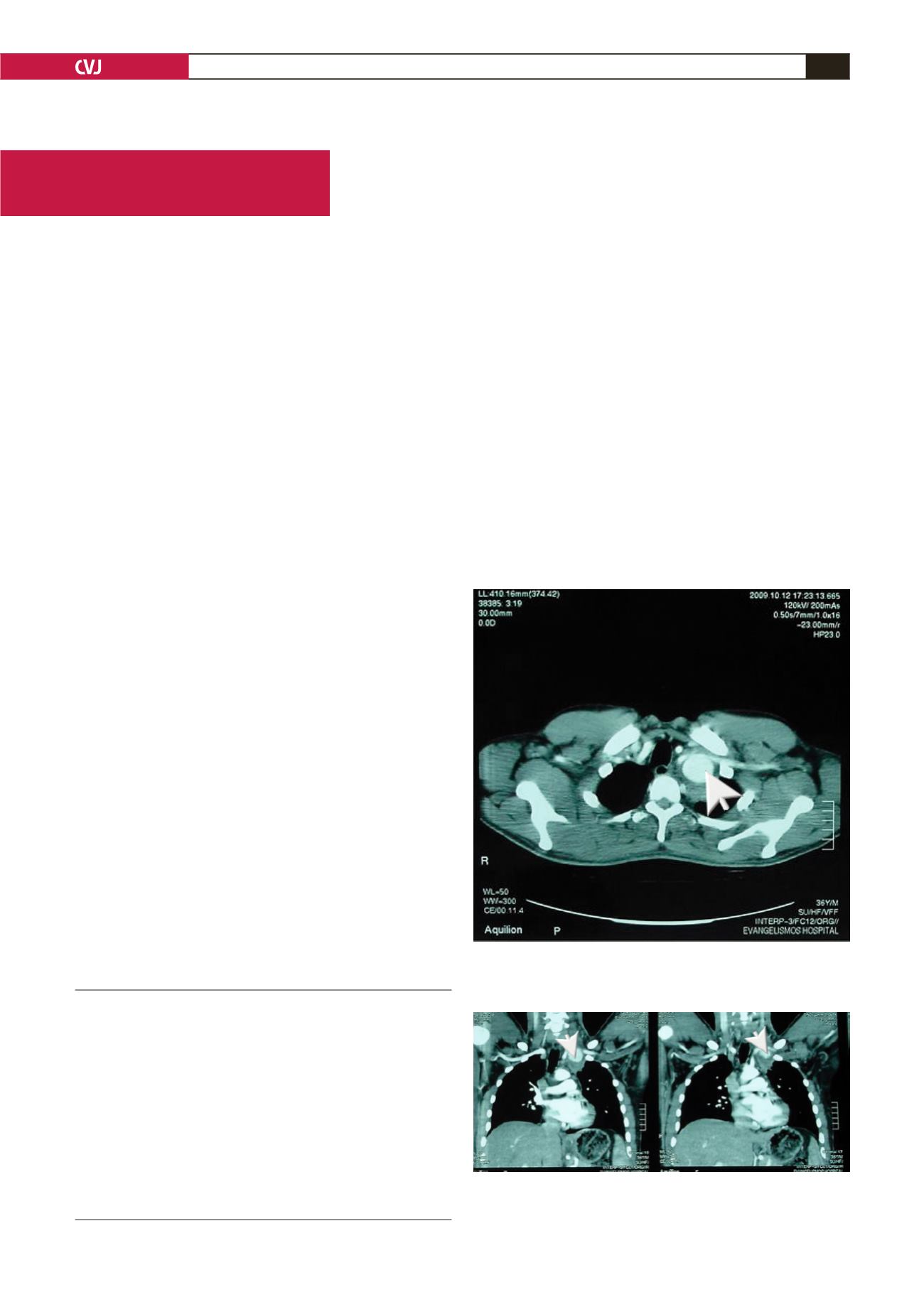
A chest computed tomography (CT) scan revealed a
solid intraparenchymal mass at the apex of the left lung. CT
angiography showed a giant intrapulmonary haematoma due to
a subclavian artery leak (Figs 1, 2).
An emergency left lateral thoracotomy was performed. The
apex of the lung was separated from the rest of the lung with
a linear staple. The subclavian artery was controlled distal
to its origin at the aortic arch. The lung apex was dissected
extrapleuraly until the subclavian artery was seen. The subclavian
artery was distally controlled just before its exit at the thoracic
outlet above the first rib. Resection of the subclavian artery was
technically demanding because several branches that originate
distal to the vertebral artery were difficult to find and control.
Thoracic Surgery Department, Sismanogleio General
Hospital, Athens, Greece
A LIOULIAS, MD, PhD
P MISTHOS, MD, PhD,
J KOKOTSAKIS, MD, PhD
P DROSOS, MD
D PAVLOPOULOS, MD
Third Department of Pneumonology, Sismanogleio General
Hospital, Athens, Greece
N KARAGIANNIDIS, MD, PhD
Department of Anaesthesia, Sismanogleio General Hospital,
Athens, Greece
M MITSELOU, MD
Fig. 1. CT angiography on the transverse plane, show-
ing a giant intrapulmonary haematoma (arrow) due to a
subclavian artery leak.
Fig. 2. CT angiography on the coronal plane, showing a
giant intrapulmonary haematoma (arrow) due to a subcla-
vian artery leak.


