CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 5, June 2012
AFRICA
e11
Case Report
Repair of a right coronary artery arising from the
pulmonary artery
ADEM GULER, MEHMET ALI SAHIN, CELALETTIN GUNAY, ARTAN JAHOLLARI, HARUN TATAR
Abstract
We present here the fourth patient in the literature, over the
age of 50 years old, with an abnormal right coronary artery
arising from the pulmonary artery, who was successfully
treated with surgery. Pre-operative computerised tomogra-
phy (CT) angiography revealed an abnormal right coronary
artery arising from the pulmonary artery. The right coro-
nary artery was surgically transposed from the pulmonary
artery to the ascending aorta with the aid of cardiopulmo-
nary bypass. The patient had an uneventful postoperative
course and the corrected anatomy was documented by post-
operative CT angiography.
Keywords:
anomalous right coronary artery, coronary malfor-
mation, ARCAPA
Submitted 13/4/10, accepted 12/9/11
Cardiovasc J Afr
2012;
23
: e11–e13
DOI:10.5830/CVJA-2011-054
Anomalous origin of the right coronary artery from the pulmonary
artery (ARCAPA) is a rare congenital coronary malformation.
1
In contrast to the Bland–Garland–White syndrome (anomalous
left coronary artery from the pulmonary artery, ALCAPA), most
patients with ARCAPA remain asymptomatic.
2,3
Although the
course of the disease has been considered benign, case reports
of sudden cardiac death do exist. Successful surgical repair
basically depends on re-establishment of a bi-coronary system.
4
We present here the fourth case in the literature of a patient over
the age of 50 years who was treated successfully with surgery.
Case report
A 51-year-old man had been admitted to hospital with a history
of syncope and complaints of palpitations and dyspnoea on
effort since childhood. No pathology was found on physical
examination. There was no murmur on cardiac auscultation.
The ECG revealed Q waves and negative T waves in the inferior
leads. The chest X-ray was normal. Cardiac enzymes were within
the normal range.
Transthoracic echocardiography revealed advanced
hypokinesia of the posterior, inferior and mid-basal septum,
minimal mitral regurgitation and decreased left ventricular
ejection fraction (45%). The left ventricle’s internal diameter in
diastole (LVIDd) was 57 mm.
Coronary angiography revealed markedly dilated and tortuous
coronary arteries. The right coronary artery arose from the
pulmonary trunk and had collateral filling from the left coronary
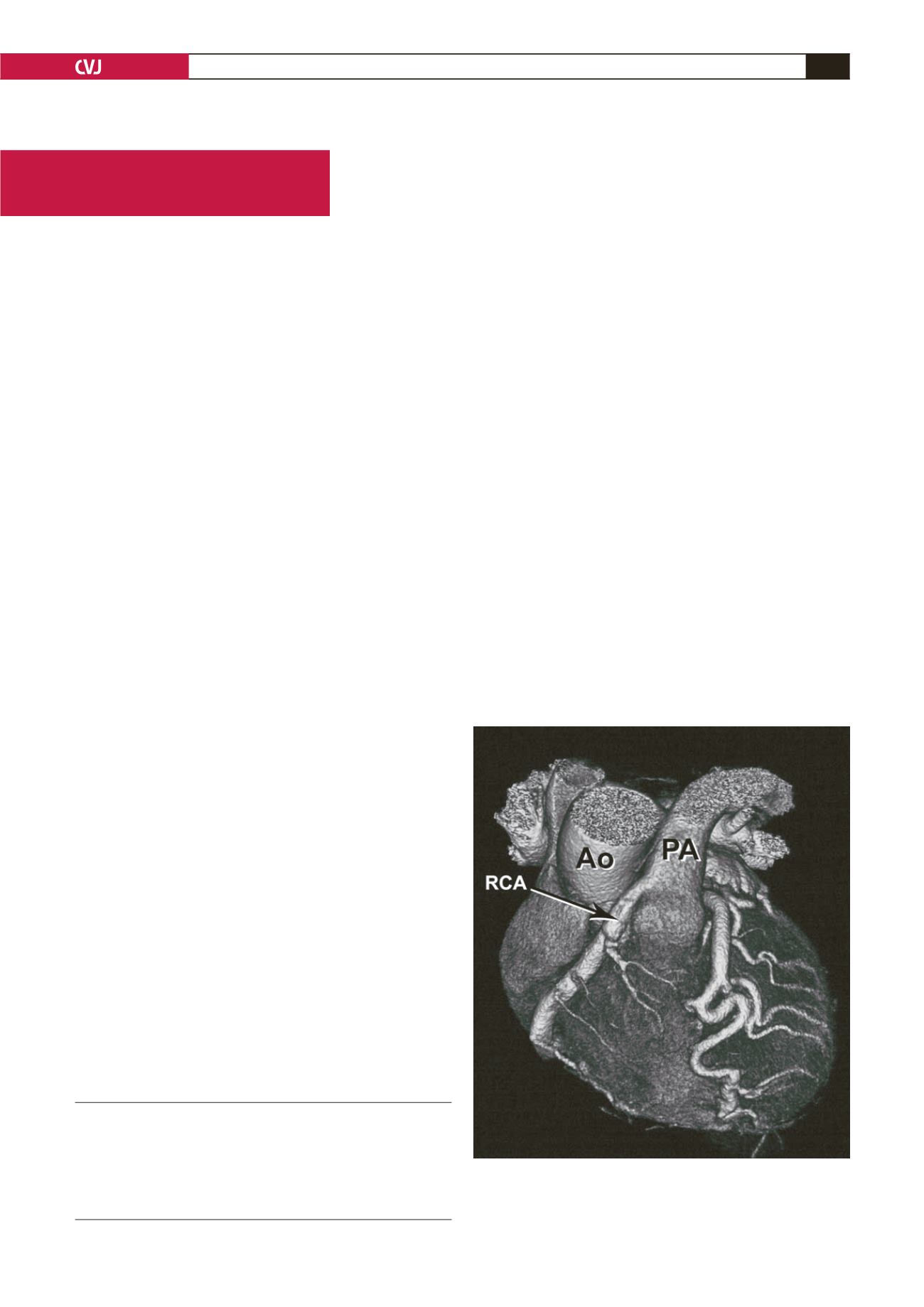
system. Computerised tomography (CT) angiography was
applied for anatomical imaging and ARCAPA was confirmed
(Fig. 1). The ectopic ostium of the RCA was from the right
anterior pulmonary cusp.
Surgical technique
After a median sternotomy and pericardiotomy, cannulas for
cardiopulmonary bypass (CPB) were placed into the right atrium
and ascending aorta. The left anterior descending artery (LAD)
was markedly dilated and tortuous. The aorta and pulmonary
Department of Cardiovascular Surgery, Gülhane Military
Medical Academy, Etlik, Ankara, Turkey
ADEM GULER, MD
MEHMET ALI SAHIN, MD,
CELALETTIN GUNAY, MD
ARTAN JAHOLLARI, MD
HARUN TATAR
Fig. 1. Pre-operative CT angiography (three-dimensional
reconstruction) showing the abnormal right coronary
artery arising from the pulmonary artery. RCA: right coro-
nary artery, Ao: aorta, PA: pulmonary artery.


