CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 5, June 2012
e12
AFRICA
trunk were separated from each other. After institution of
CPB, an aortic cross clamp was applied and cold crystalloid
cardioplegia was administered.
The origin of the anomalous right coronary artery arising
from the right anterior aspect of the main pulmonary trunk was
dissected and transected from the pulmonary trunk. The defect
on the pulmonary trunk was repaired with a primary closure. A
hole was created with a 5-mm punch slightly to the left anterior
aspect of the ascending aorta, and the right coronary artery was
anastomosed there. A standard decannulation procedure was
performed.
After sternal and wound closure, the patient was transferred
to the cardiac surgical intensive care unit, and the following day
to the postoperative ward. After an uneventful postoperative
course, the patient was discharged on the sixth postoperative day.
During the follow up, the patient was asymptomatic. No change
in cardiac enzymes was observed. The corrected anatomy was
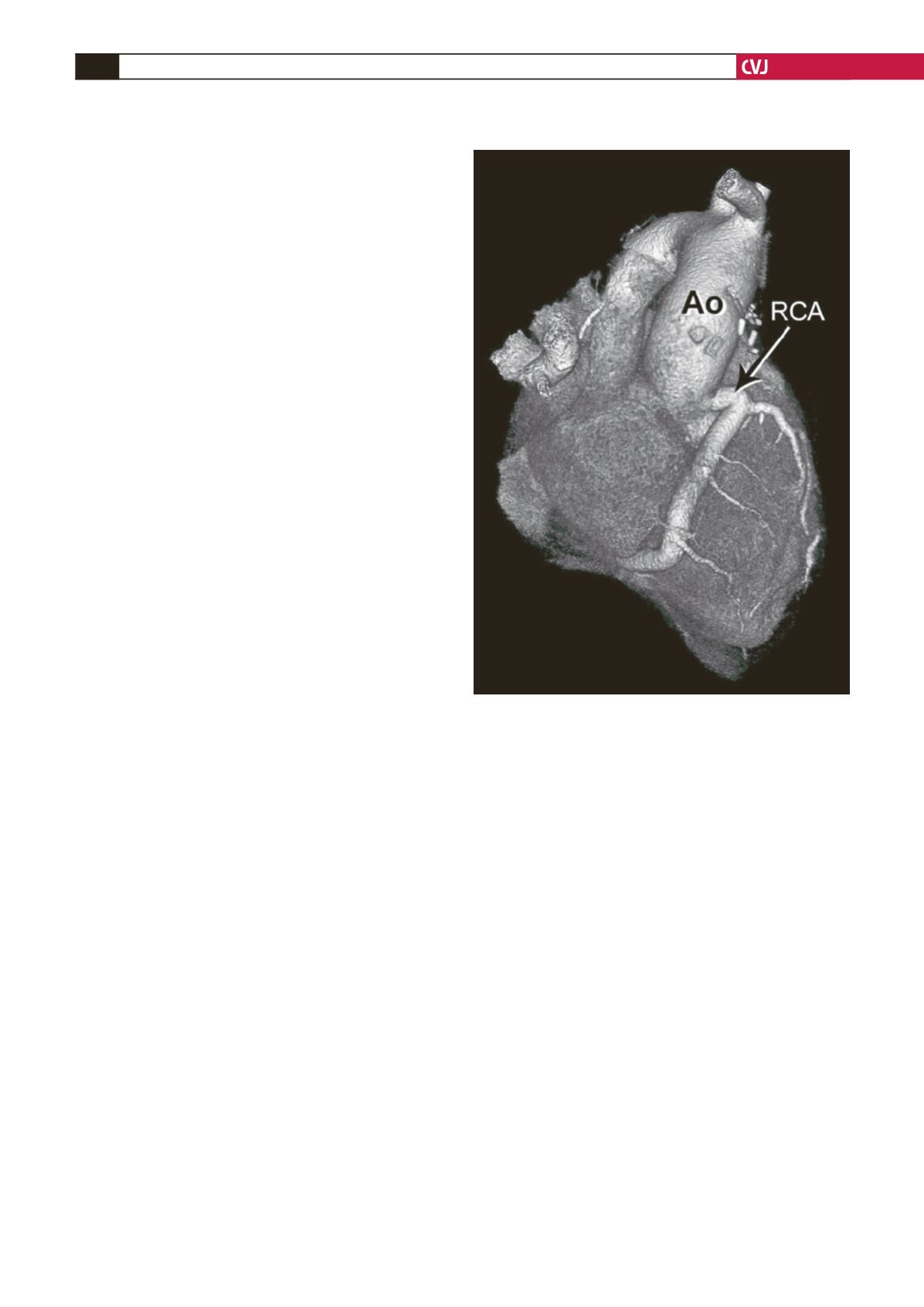
documented by postoperative CT angiography (Fig. 2).
At 24 months after the procedure, the patient had a normal
treadmill test and echocardiography revealed a hypokinetic
inferior septum, increased left ventricle ejection fraction (54%),
minimal mitral regurgitation and a LVIDd of 54 mm.
Discussion
Anomalous origin of the coronary arteries from the pulmonary
artery is a rare congenital cardiac anomaly. Its incidence is one
in 30 000 to 300 000 live births.
5-8
ALCAPA is the most common
form of this type of anomaly, accounting for more than 90% of
cases and 0.5% of all congenital cardiac anomalies.
6
ARCAPA is
very rare compared to ALCAPA.
7,
9
The only predictable morphological finding is an increase in
the size of the left main coronary artery and its branches, and an
increase in the size of the RCA with thinning of its wall.
7
As in
our patient, the ectopic ostium of the RCA originates from the
right anterior pulmonary cusp in the majority of cases. Right
coronary artery dominance is usual. The flow pattern in the
collateral circulation between the left coronary system and the
RCA is similar to that of coronary atherosclerosis. The major
source of collateral circulation to the RCA is septal branches of
the LAD.
10
In this anomaly, left and right ventricular functions are not
corrupted and findings of impaired cardiac function do not
occur.
10
Generally there are no signs of myocardial ischaemia,
while symptoms and clinical findings of congestive heart failure
may be present only in rare paediatric cases.
11
In an autopsy series of nine cases, congestive heart failure
was found in a two-year-old child who died without any previous
symptoms, in an 11-year-old patient who died from cardiac
arrest, and in a 72-year-old male patient. There were no signs
of cardiac pathology or impaired cardiac function reported in
the remaining six patients.
7
In 30 of these 58 patients, other than
the autopsy cases, the anomaly was primarily diagnosed with
angiography. At the time of diagnosis their ages varied between
one day and 90 years old.
12
The real incidence of this anomaly is probably higher than
reported because a large number of patients are asymptomatic.
This is opposite to what is seen in ALCAPA. Findings of mitral
regurgitation and myocardial infarction, often seen in the early
ages of ALCAPA, are not encountered in this anomaly.
This anomaly shows different clinical signs when it becomes
symptomatic. Dyspnoea develops in 17% of patients, while
fatigue occurs in 13%, angina in 17%, mitral regurgitation in
9%, congestive heart failure in 30% and cardiac arrest in 17%
of patients.
3
Objective findings were not specific in most of
the cases, except in those who had angiography. Ischaemia was
present in 40% of patients.
In adults, this anomaly is typically diagnosed due to a cardiac
murmur or during angiography performed for other reasons.
10
However, hidden ischaemia, revealed from a positive stress
test and angina (mostly atypical angina) may develop in some
patients.
13
Although an ECG is helpful in the investigation of ALCAPA,
it does not play a meaningful role in diagnosing right coronary
artery anomaly. Generally there are no ischaemic changes and
ventricular hypertrophy is usually absent or borderline. The heart
silhouette in telecardiographymay be slightly increased.Although
diagnostic findings may be present on echocardiography, there
has been no report in the literature of any case diagnosed
with only this method. Besides 12 cases diagnosed at autopsy,
three cases were diagnosed intra-operatively, 25 cases with
angiography, while in five cases, angiography was performed
after the echocardiographic findings suggested this anomaly.
It is not enough to show that the right coronary artery does
not originate from the aortic root, it is important to determine
Fig. 2. Postoperative CT angiography (three-dimensional
reconstruction) showing the right coronary artery trans-
posed to the ascending aorta. RCA: right coronary artery,
Ao: aorta.


