CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 1, February 2012
AFRICA
53
cular risk stratification in contemporary
populations with diabetes who are already
receiving many risk-reducing therapies.
It would be interesting if this acceptable
performance was demonstrated in other
validation studies, and that the uptake of
the model be shown to improve decision
making and the outcomes of care.
Dr AP Kengne
South African 2012 guidelines for hypertension therapy
Therapeutic options in hypertension management: 2012 guidelines from the Southern African
Hypertension Society
Introduction
This guideline should perhaps be called
SAHS 5,
1
in keeping with other hyperten-
sion organisations’ approach of regarding
guideline development as a continuum.
As new studies emerge, guidelines are
updated as a general reference for clinical
practice.
South African guidelines have been
issued since 1995,
2
with the first guide-
lines being endorsed by the Medical
Association of South Africa and the
Medical Research Council. The first
guideline was directed at achieving a
target blood pressure (BP) of systolic
(SBP) 140–159 mmHg and diastolic
(DBP) 90–94 mmHg, with minimal or
no drug side effects. Subsequent guide-
lines were issued in 2001,
3
2003
4
(partial
update), 2006,
5
and now the 2012 guide-
lines have been released, all targeting
blood pressure to lower levels of 140/90
mmHg.
Cost effectiveness has always been
a feature of South African hyperten-
sion treatment guidelines, but the new
2012 guidelines have adopted a different
approach to achieving cost effectiveness.
This is based on using an ‘evidence-based
approach to the estimation of cardiovas-
cular disease (CVD) risk and treating
those patients at highest or moderate
risk, and identifying those (at lower and
moderate risk) who can benefit most from
lifestyle and drug interventions at the
lowest cost, given the country’s limited
resources’.
In reviewing the development of
South African guidelines, it is clear that
they provoke considerable debate and
comment. A recent South African MRC
6
review of clinical practice guidelines
within the Southern African Development
Community notes that the South African
hypertension guidelines (reviewed only
up until 2006) are in high agreement
with current best evidence but noted the
poorer score in the ‘editorial independ-
ence domain’, reflecting on the poor
reporting of potential conflicts of inter-
est of participating experts. The authors
in this Medical Research Council study
note that ‘Although the absence of these
declarations does not necessarily imply
that inappropriate influences guided the
final recommendations, the presence of
such declarations ensures that a guideline
can be considered trustworthy’.
Rationale for cardiovascular risk
assessment
As this guideline seeks to place effec-
tive treatment in the realm of managing
individuals with the greatest potential
to benefit from treatment, cardiovascu-
lar disease risk assessment is pivotal.
The guideline recognised that interna-
tional risk-assessment systems and charts
do have shortcomings, particularly with
regard to developing countries such as
South Africa.
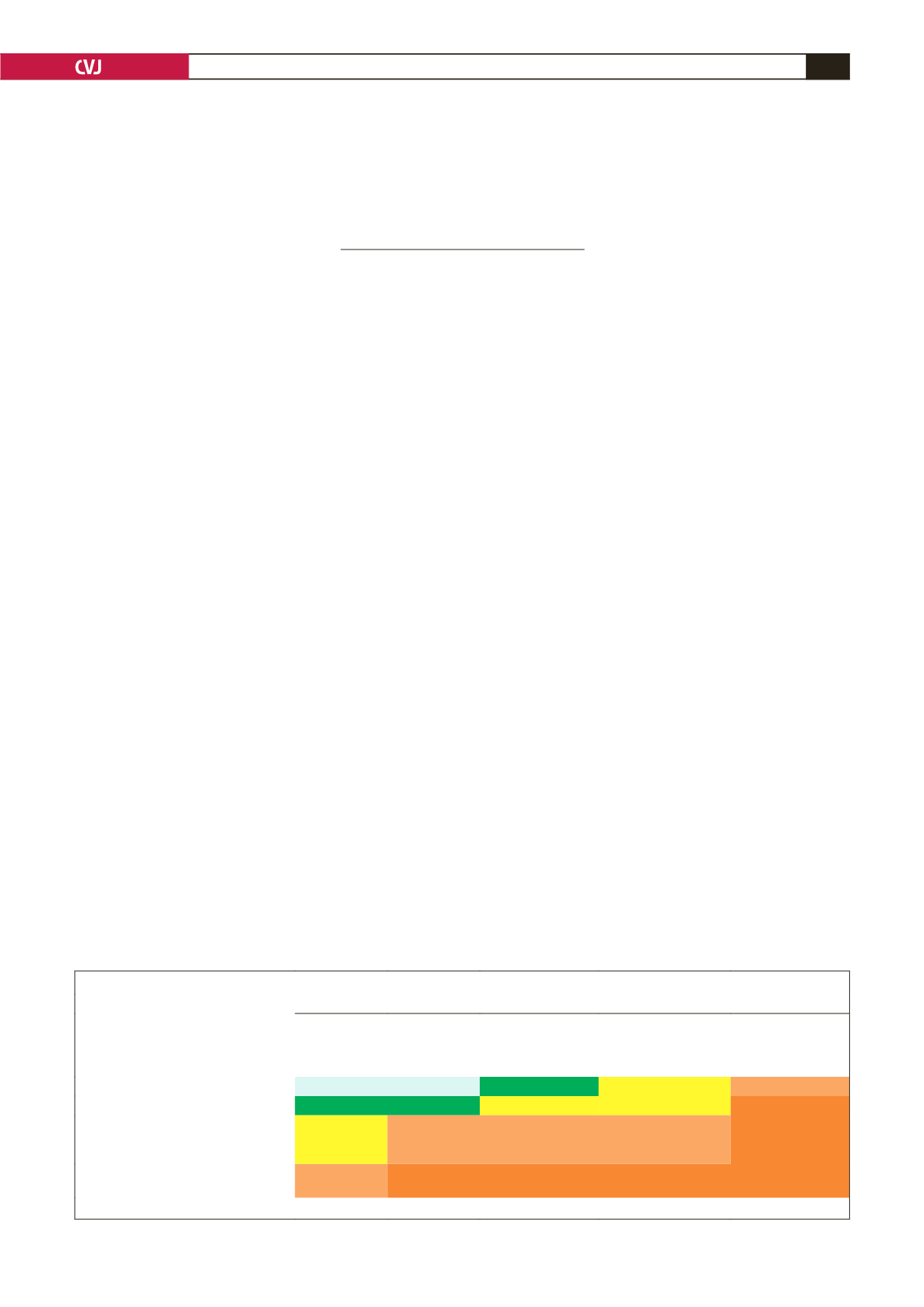
It bases these guidelines, until a
national consensus on a different model
emerges from all stake-holders (profes-
sionals, providers, government and
healthcare funders), on the risk strati-
fication from the ESH/ESC guidelines
7
(Table 1). Using this risk stratification,
the Guideline Committee has developed
a management flow diagram, cited as an
adaptation from the WHO cardiovascu-
lar disease risk-management approach
for low–medium resource settings (Fig.
1). The definition of major risk factors,
target-organ disease and associated clini-
cal conditions (ACC) is adapted from the
current ESH/ESC guidelines (Table 2).
Considerable guidance is given in
TABLE 1. STRATIFICATION OF RISKTO QUANTIFY PROGNOSIS*
BP (mmHg)
Other risk factors and disease history
Normal
SBP 120–129
or DBP 80–84
High normal
SBP 130–139
or DBP 85–89
Stage 1
Mild hypertension
SBP 140–159
or DBP 90–99
Stage 2
Moderate hypertension
SBP 160–179
or DBP 100–109
Stage 3
Severe hypertension
SBP > 180
or DBP > 110
No other major risk factors
Average risk Average risk Low added risk Moderate added risk High added risk
1–2 major risk factors
Low added risk Low added risk Moderate added risk Moderate added risk Very high added risk
≥
3 major risk factors or target-organ
disease or diabetes mellitus or
metabolic syndrome
Moderate
added risk
High added risk High added risk
High added risk Very high added risk
Associated clinical conditions
High added risk Very high
added risk
Very high added risk Very high added risk Very high added risk
* Based on the ESH/ESC guidelines.


