CARDIOVASCULAR JOURNAL OF AFRICA • Vol 23, No 1, February 2012
54
AFRICA
the guidelines to correct blood pressure
measurement, the value of ambulatory
blood pressure measurement and the
requirement of repeated blood pressure
measurements, performed on three sepa-
rate occasions within a period of two
months, to confirm a diagnosis of hyper-
tension at a SBP
≥
140 mmHg and/or a
DBP
≥
90 mmHg. Lifestyle modifica-
tion in hypertension treatment, regard-
less of blood pressure level is stressed,
and the guidelines support the South
African Department of Health strategy for
a healthy lifestyle.
Drug therapy
At the outset, the guidelines point out that
patients should not be changed frequently
from one generic to another in the same
class, solely because of a lower price.
While cost-containment is an issue, the
guidelines note that best-practice recom-
mendations should be stated clearly and if
a compromise has to be introduced, based
on limited resources, ‘this (choice) should
be made deliberately and transparently’.
1
In this case, one presumes that the patient
will be told that the healthcare provider,
whether the state or private sector, has
limited his/her access to ‘best-practice
medication’.
The implementation of drug therapy is
recommended in low-risk patients whose
blood pressure remains above 140/90
mmHg despite six to 12 months of obser-
vation and lifestyle recommendations. For
moderate risk, the time period of being
above target is three to six months.
Risk stratification is vital to the guide-
lines and therefore the importance of
conditions favouring or disfavouring a
therapy’s usage will determine best-prac-
tice therapy in the majority of treated
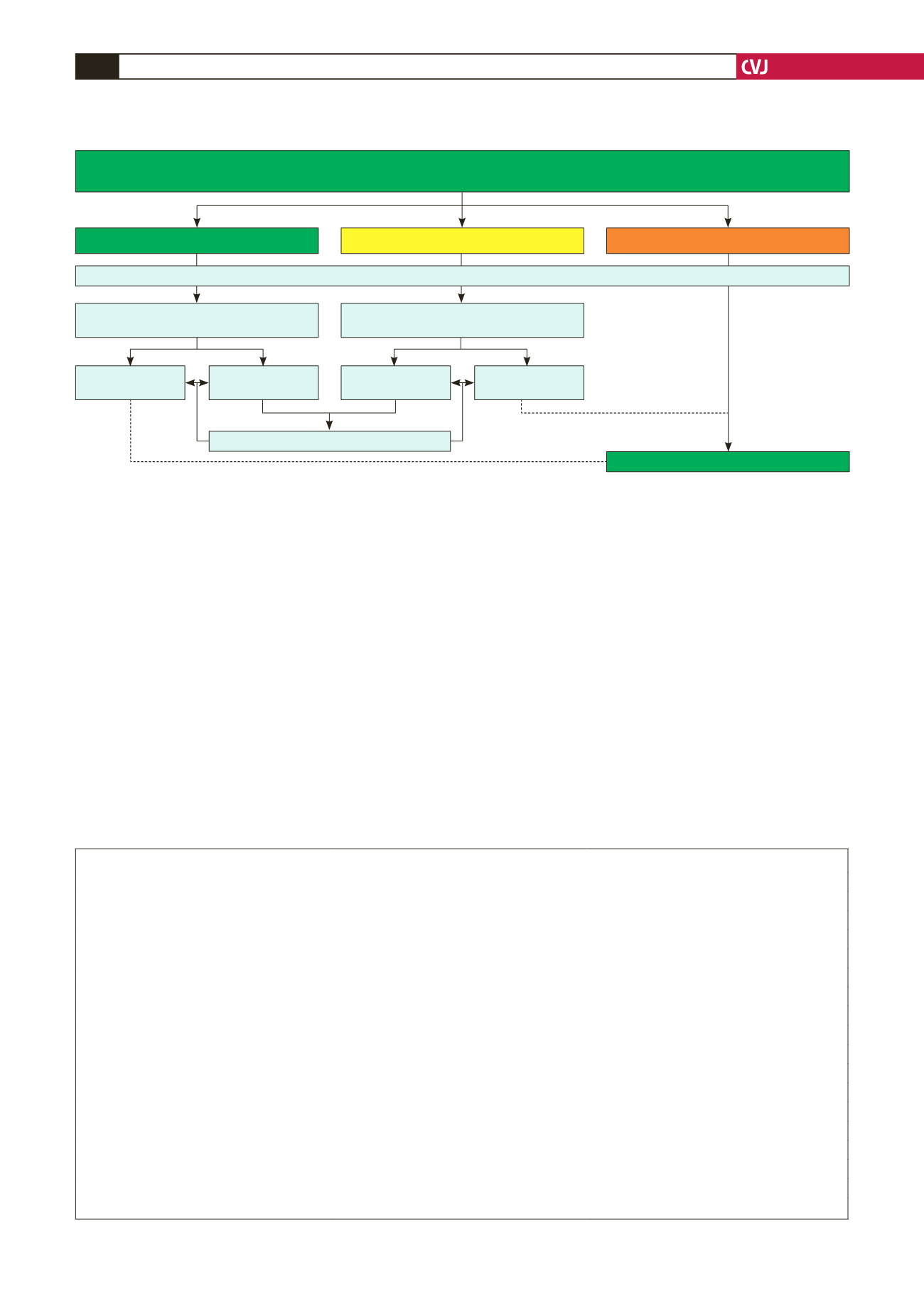
Fig. 1. Southern African hypertension management flow diagram based on added CVD risk (adapted from the WHO CVD risk-manage-
ment package for low–medium resource settings).
STRATIFY ACCORDING TO ADDED RISK (as in risk chart Table 1)
BP LEVEL + MAJOR RISK FACTORS + TOD + ACC
LOW ADDED RISK
Monitor BP and other risk factors
for 3–6 months
MODERATE ADDED RISK
HIGH/VERY HIGH ADDED RISK
Monitor BP and other risk factors
for 6–12 months
SBP
≥
140 or
DBP
≥
90 mmHg
SBP
<
140 and
DBP
<
90 mmHg
SBP
<
140 and
DBP
<
90 mmHg
SBP
≥
140 or
DBP
≥
90 mmHg
Continue to monitor
BEGIN DRUG TREATMENT
LIFESTYLE MODIFICATION AS APPROPRIATE
TABLE 2. MAJOR RISK FACTORS, TARGET-ORGAN DAMAGE (TOD) ANDASSOCIATED CLINICAL CONDITIONS (ACC)*
Major risk factors
TOD
ACC
Levels of SBP and DBP
LVH: based on ECG
Coronary heart disease
Smoking
Sokolow-Lyon
>
38 mm
Heart failure
Dyslipidaemia
Cornell
>
2 440 mm/ms
Chronic kidney disease
Total cholesterol
>
5.1 mmol/l, OR
Microalbuminuria
albuminuria
>
30 mg/mmol, OR
LDL
>
3 mmol/l, OR
albumin creatine ratio 3–30 mg/mmol
creatinine
>
133
μ
mol/l (men)
HDL
<
1 (men) and
<
1.2 mmol/l (women)
Slightly elevated creatinine:
creatinine
>
124
μ
mol/l (women)
Diabetes mellitus
115–133
μ
mol/l (men)
Stroke or TIA
Men aged
>
55 years
107–124
μ
mol/l (women)
Peripheral arterial disease
Women aged
>
65 years
Advanced retinopathy:
Family history of early-onset CVD
haemorrhages, OR
Men aged
<
55 years
exudates
Women aged
<
65 years
papilloedema
Waist circumference
Men
≥
94 cm
Women
≥
80 cm
Exceptions are South Asians and Chinese: men
>
90 cm and women
>
80 cm
*Adapted from the ESH/ESC guidelines.


